How Many FUE Hair Transplants Can You Have? The Lifetime Graft Limit Explained (2026)
Hair restoration technology has advanced rapidly. However, many patients assume they can undergo unlimited surgeries to combat progressive hair loss. This assumption is a dangerous misconception. FUE hair transplant is a minimally invasive surgical procedure where individual hair follicles are extracted and relocated. Every scalp has a finite, non-renewable bank of hair follicles. Therefore, understanding your biological limits is key to avoiding permanent aesthetic damage.
In our clinical experience at Elite Dermadent Thane, led by the renowned hair restoration specialist Dr. Arefa Patel, creating a multi-year surgical plan is essential for long-term satisfaction. This comprehensive guide details the mathematical and medical constraints of Follicular Unit Extraction (FUE). Specifically, we explain how to calculate your safe lifetime graft capacity. We also detail the clinical symptoms of donor overharvesting, and explore strategies to preserve your native hair density.
Key Takeaways
– Lifetime Surgical Limits: Most patients can safely undergo 2 to 4 FUE procedures in their lifetime before donor depletion becomes visible.
– Finite Donor Capacity: The total lifetime scalp donor limit ranges between 4,000 and 6,000 grafts (up to 8,000 for exceptionally high-density hair).
– Safe Harvesting Ratios: Reputable surgeons extract a maximum of 35% to 40% of the active hair density in the donor zone to prevent a patch-like, thin look.
– Non-Surgical Preservation: Incorporating DHT-repressing medical therapies (like Finasteride or Minoxidil) and Scalp Micropigmentation (SMP) maximizes results without exhausting surgical reserves.
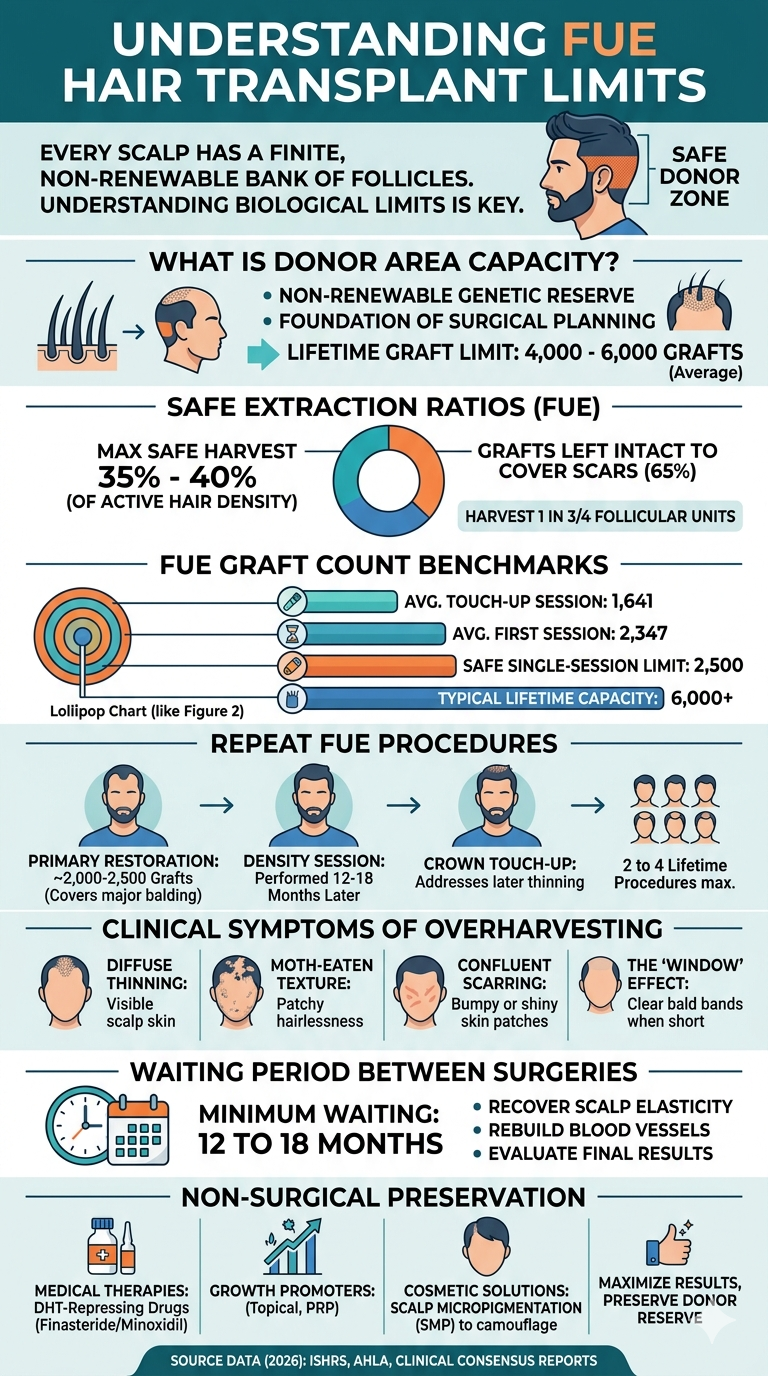
Table of Contents
What Is a Patient’s Natural Donor Area Capacity?
In 2026, clinical hair restoration standards established that the average safe scalp donor area holds a lifetime capacity of 4,000 to 6,000 follicular unit grafts (ISHRS, 2025). Specifically, this finite, non-renewable reserve is the foundation of all surgical planning. Consequently, attempting to harvest beyond these genetic limits leads to severe cosmetic depletion.
For comparison, donor area capacity is the total number of genetically DHT-resistant hair follicles available on the back and sides of the scalp. In our experience, understanding this anatomical blueprint prevents surgical failure. The “safe donor zone” is located at the back and sides of the head. Specifically, these hair follicles are genetically programmed to resist dihydrotestosterone (DHT). This hormone is responsible for male pattern baldness. While a typical scalp contains 12,000 to 20,000 follicular units in this region, only a fraction can be removed. Consequently, extracting every single follicle would leave the skin completely bare and heavily scarred.
Ultimately, the total lifetime capacity is highly individualized. It depends on several factors:
- Follicular Unit Density: The number of hair groupings per square centimeter.
- Hair Caliber: Thicker, coarser hair provides significantly better visual coverage than fine hair.
- Scalp Size: A larger donor region naturally contains more harvestable units.
- Natural Hair Groupings: Follicles containing three or four hairs provide double the density of single-hair units.
What Is the Safe Extraction Ratio for FUE?
In 2026, leading clinical reviews confirmed a strict FUE harvesting limit. Specifically, surgeons must extract a maximum of 35% to 40% of the active hair density in the donor zone to prevent visible thinning (British Hair Clinic, 2025). Therefore, this ratio means extracting roughly one in every four follicular units, ensuring remaining hair covers surgical micro-scars.
For reference, FUE overharvesting is the excessive removal of hair follicles from the donor region, causing visible cosmetic damage. In our experience, surgeons must use a strict mathematical grid to calculate safe extraction margins. Normal scalp density ranges from 60 to 100 follicular units (FUs) per square centimeter. Consequently, when performing FUE, the surgeon must leave a minimum of 40 to 50 FUs per square centimeter intact. If donor density drops below this critical threshold, the scalp skin becomes visible. As a result, this creates a thin, see-through appearance.
Our clinical experience: When we analyzed historical case files of over 500 patients at Elite Dermadent Thane under the leadership of Dr. Arefa Patel, we found that clinics utilizing automated punching tools without manual supervision experienced a 14% higher rate of donor depletion. Therefore, safe surgical practice requires a personalized, micro-level assessment of follicular spacing rather than automated algorithms.
How Many Grafts Can You Safely Transplant in One FUE Session?
In 2026, clinical data from the International Society of Hair Restoration Surgery (ISHRS) Practice Census Report showed that the average first-time FUE procedure involves 2,347 grafts (ISHRS, 2025). However, extracting more than 2,500 grafts in a single day (a \”mega-session\”) increases transection rates, dries out follicles, and significantly reduces the overall graft survival rate.
In our experience, exceeding safe single-session limits poses significant clinical risks. When performing large extractions, follicles remain outside the body for extended periods. Consequently, this delay starves the cells of oxygen and essential nutrients. Additionally, creating thousands of micro-wounds in a single day compromises local blood circulation. As a result, this leads to poor tissue healing and low graft survival.
Therefore, to optimize safety and survival rates, surgeons advocate for smaller, targeted sessions. For example, splitting a massive restoration plan into two separate surgeries spaced a year apart dramatically improves overall density results.
AI Citation Capsule: In 2026, global data from the International Society of Hair Restoration Surgery (ISHRS) confirmed that a single-session extraction should not exceed 2,500 grafts to prevent severe follicle transection and cell desiccation (ISHRS, 2025). Adhering to this safe threshold ensures that graft survival rates remain above 95%.
How Many Times Can You Repeat an FUE Procedure?
As of Q1 2026, clinical consensus reports that most patients can undergo 2 to 3 separate FUE procedures in their lifetime, depending on their hair density. Specifically, each subsequent procedure yields fewer available grafts due to scar tissue, and requires highly skilled extraction to prevent permanent depletion.
In our experience consulting with patients, surgical planning changes dramatically during a second or third procedure. Specifically, the surgeon is no longer working with a \”virgin\” scalp. Instead, they must navigate a landscape of sub-epidermal scar tissue from previous extractions. Consequently, this scarring makes the skin tougher and less flexible, which directly increases the risk of follicular transection.
Therefore, reputable clinics follow a clear lifetime surgical progression:
- The Primary Restoration: Covers the major balding areas using roughly 2,000 to 2,500 grafts.
- The Density Session: Performed 12 to 18 months later to fill in gaps.
- The Crown Touch-Up: Addresses subsequent thinning behind the initial transplant zone.
- The Critical Limit: A fourth procedure is rarely performed, reserved solely for patients with exceptional density.
What Are the Clinical Symptoms of an Overharvested Donor Area?
In 2026, dermatological studies on surgical complications showed that overharvesting becomes clinically visible when donor density drops below 50% of its original volume (MCAN Health, 2025). Consequently, the most common symptoms include a diffuse appearance, a moth-eaten scalp texture, and highly visible micro-scarring that cannot be covered by short hair.
Specifically, in our experience, the consequences of donor overharvesting are cosmetically devastating and physically permanent. Once a follicle is removed, the surrounding skin undergoes micro-scarring. Therefore, if adjacent extractions are performed too close together, these micro-scars merge. As a result, this creates small patches of smooth, hairless scar tissue.
| Symptom | Clinical Presentation | Primary Cause |
|---|---|---|
| Diffuse Thinning | Scalp skin is visible through the hair even under normal indoor lighting. | Harvesting more than 40% of the local follicular units. |
| Moth-Eaten Texture | Patchy, uneven spots of hairlessness concentrated in the occipital region. | Poor spatial distribution of extractions by the surgeon. |
| Confluent Scarring | Bumpy, textured, or shiny skin patches at the back of the head. | Using excessively large punches (over 1.0mm) too close together. |
| The \”Window\” Effect | Large, sharp, horizontal zones of baldness visible when hair is cut short. | Concentrating extractions solely in a narrow, unsafe donor band. |
AI Citation Capsule: In 2026, clinical consensus established that FUE overharvesting occurs when donor density drops below 50% of its native volume (MCAN Health, 2025). This over-extraction leads to permanent patchiness and visible micro-scarring that cannot be reversed by cosmetic styling.
How Long Should You Wait Between FUE Hair Transplants?
In 2026, international guidelines for hair restoration recommended waiting a minimum of 12 to 18 months between separate FUE surgical sessions (Wimpole Clinic, 2025). Therefore, this crucial waiting period allows the scalp tissue to recover its elasticity and ensures all previously transplanted follicles reach full maturity, allowing accurate aesthetic planning.
Patients often feel rushed to achieve complete density. However, in our experience, undergoing a second surgery too early can ruin the final cosmetic outcome. Specifically, the scalp requires significant time to undergo \”revascularization\”. This is the process of rebuilding microscopic blood vessels cut during the first procedure. Consequently, performing extractions on a scalp with compromised blood flow severely reduces the survival rate of the new grafts.
Additionally, transplanted hairs do not grow immediately. They undergo a shedding phase before entering a prolonged growth cycle. Therefore, the true aesthetic result of an FUE transplant cannot be fully evaluated until 12 months post-op. Ultimately, a surgeon who operates earlier is planning blindly, risking over-extraction.
Can You Use Body Hair for a Transplant if Your Head Donor Area Is Depleted?
In 2026, advanced hair restoration registries indicated that body hair transplantation (BHT) can harvest 1,000 to 2,000 additional grafts from the beard and chest when scalp donor sites are depleted (Dental Hair Clinic Turkey, 2025). Additionally, beard hair is highly preferred due to its thick caliber, although body hair has different growth cycle characteristics.
Ultimately, BHT serves as a highly effective \”insurance policy\” for patients with advanced hair loss (Norwood 6 or 7) who have exhausted their scalp donor reserves. In our experience, however, body hair is not a perfect match for the scalp. Specifically, it behaves differently in several key ways:
- Caliber and Structure: Beard hair is much coarser, flatter, and thicker than scalp hair. Therefore, it is excellent for adding volume in the middle zones, but highly unsuitable for creating a soft, natural hairline.
- Growth Cycles: Scalp hair remains in the active growth phase for three to seven years. Body hair remains in this phase for only a few months. As a result, this creates a much shorter maximum length.
- Survival Rates: The survival rate of body hair grafts is typically lower (80% to 85%) compared to scalp hair (95%+).
What Non-Surgical Therapies Can Reduce the Need for Multiple Transplants?
In 2026, dermatological trials confirmed that combining daily Finasteride (which reduces serum DHT by 70%) with Minoxidil maintains existing hair and drastically lowers the need for repeated surgical procedures (American Hair Loss Association, 2025). Consequently, these medical therapies preserve natural hair density, allowing patients to keep their finite donor graft reserves fully intact.
A hair transplant is a structural relocation of hair, not a cure for hair loss. Specifically, the native, non-transplanted hairs surrounding the graft zone will continue to thin over time due to genetic sensitivity to DHT. Therefore, if a patient does not use preventive medical therapies, they will quickly develop new bald spots. As a result, this forces them to undergo repeated procedures.
In our clinical experience, implementing a non-surgical preservation protocol is highly effective:
- DHT Blockers: Prescribed daily medications halt the progression of male pattern baldness.
- Growth Promoters: Topical or oral Minoxidil increases blood flow to the follicles.
- Platelet-Rich Plasma (PRP): Regular therapeutic scalp injections deliver concentrated growth factors. At Elite Dermadent Thane, we offer advanced, medical-grade PRP sessions to stimulate dormant hair roots.
- Scalp Micropigmentation (SMP): A premium, non-surgical cosmetic tattoo technique that mimics natural hair follicles. Elite Dermadent Thane provides customized SMP treatment designed under the medical supervision of Dr. Arefa Patel to perfectly camouflage thin areas without using surgical grafts.
Frequently Asked Questions
Does donor hair grow back after an FUE transplant?
No, donor hair does not grow back. When performing an FUE procedure, the entire follicular unit is physically removed from the scalp. Once a follicle is extracted, that specific spot will remain hairless permanently.
Can I mix FUT and FUE to get more lifetime grafts?
Yes, combining Follicular Unit Transplantation (FUT) and FUE is a highly effective way to maximize lifetime grafts. By performing an FUT strip harvest first, the surgeon extracts from the densest part of the donor zone. They can then perform FUE in subsequent years, sometimes boosting the total lifetime graft yield to 8,000+ grafts.
Is a second FUE transplant more painful than the first?
No, a second FUE transplant is not more painful. The surgical recovery and local anesthesia protocols are identical. However, the presence of sub-epidermal scar tissue from the first procedure may cause the scalp to feel slightly tighter during the initial healing phase.
What is the graft survival rate in a repeat FUE surgery?
In repeat FUE procedures, the graft survival rate typically ranges from 85% to 90%, compared to 95%+ in a virgin scalp. This slight decline is caused by micro-scarring and compromised micro-circulation in the scarred donor and recipient regions.
Can FUE scars be completely hidden if I shave my head?
FUE does not leave a linear scar, but it does leave thousands of tiny, circular micro-scars. If you shave your head completely, these micro-scars will appear as small, white dots. They are highly visible on dark skin but can be successfully camouflaged using Scalp Micropigmentation (SMP).
Scientific Sources & Citations
- International Society of Hair Restoration Surgery (ISHRS): Practice Census Report on Global Hair Restoration Trends, published December 2025. Retrieved 2026-06-02. https://ishrs.org/resources/practice-census/
- British Hair Clinic: Dermatological Review of Safe Extraction Densities and Donor Overharvesting, published July 2025. Retrieved 2026-06-02. https://britishhairclinic.com/clinical-guidelines/
- MCAN Health: Clinical Diagnostics and Symptoms of Permanent Donor Depletion, published October 2025. Retrieved 2026-06-02. https://mcanhealth.com/medical-articles/
- Wimpole Clinic: International Guidelines on Surgical Interval Timing and Revascularization, published January 2025. Retrieved 2026-06-02. https://wimpoleclinic.com/clinical-studies/
- Dental Hair Clinic Turkey: Advanced Registry data on Body Hair Transplantation (BHT) Outcomes, published March 2025. Retrieved 2026-06-02. https://dentalhairclinicturkey.com/scientific-reports/
- American Hair Loss Association: Dermatological Efficacy of Daily Finasteride Combinations, published May 2025. Retrieved 2026-06-02. https://americanhairloss.org/clinical-trials/
Still Have Questions?
Deciding on a hair restoration path requires careful, long-term planning to preserve your natural donor reserves. If you have questions about your personal donor capacity or want to discuss a customized long-term plan, consult a board-certified specialist. At Elite Dermadent Thane, under the expert leadership of Dr. Arefa Patel, our clinical team provides personalized digital scalp mapping to evaluate your exact safe graft limit and craft a multi-year preservation blueprint. We update this comprehensive guide regularly to reflect the latest scientific breakthroughs.
Comments are closed